
Glioblastomas are the most aggressive, malignant primary tumour of the brain. They are also, unfortunately, the commonest. We have not seen any new treatments in over a decade. My group is particularly interested in focal therapies, surgery and radiotherapy. As a surgeon, we walk a tightrope between not taking enough tumour so it progresses rapidly or taking too much and damaging the normal brain. My research group focuses on identifying individualised treatment volumes to maximise tumour resection without impacting quality of life. Our research has four themes: 1. Develop imaging tools to map the extent of glioblastomas 2. Understand the impact of surgery on cognitive function and develop rehabilitation strategies to overcome neurocognitive deficits. 3. Imaging intra- and inter-tumoural heterogeneity 4. Develop machine learning tools to phenotype patients better We believe that if we can understand tumour heterogeneity, we can individualise therapy for patients.
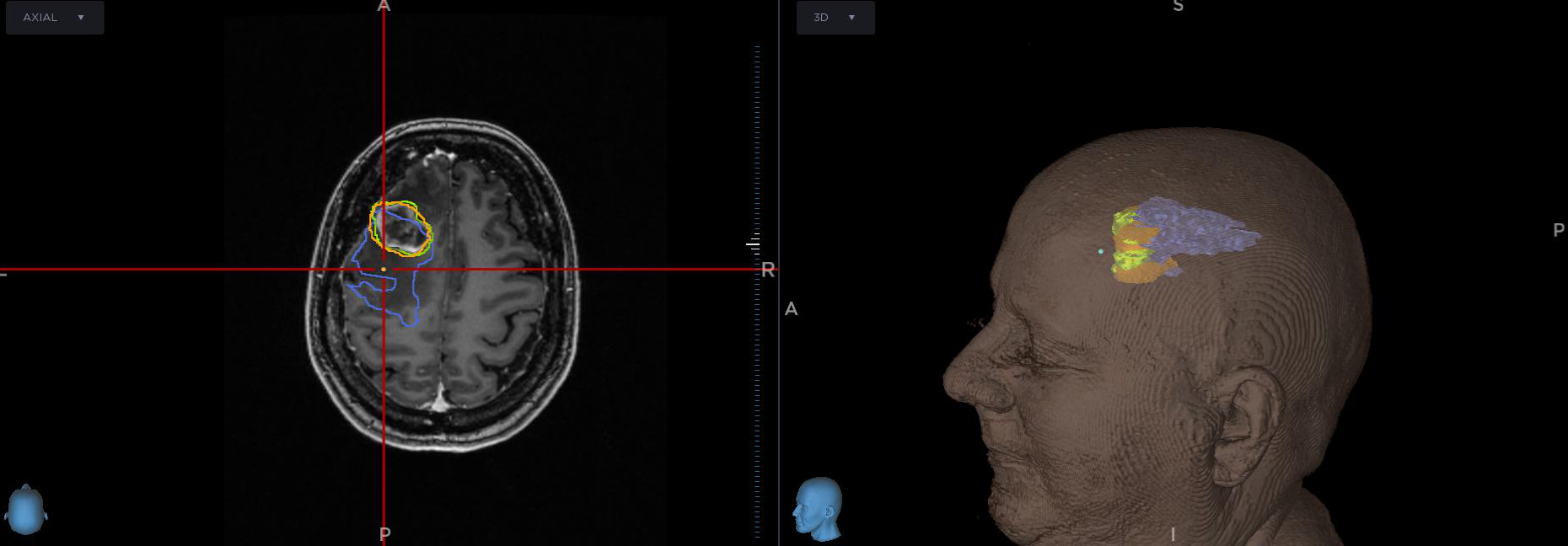
Bringing advanced imaging into the operating theatre
This is an example of incorporating advanced imaging into our surgical image-guidance system. We have outlined the contrast enhancing tumour (in green) and the [C-11]-methionine PET in orange (as the likely target to be resected with 5-ALA fluorescence). The blue is the DTI anisotropic component (q) that identifies likely residual tumour. The PRaM-GBM study has shown that this can identify where tumours will progress with sensitivities around 80% with specificity of 95%. This is now a target for biopsy (to provide biological validation) before starting an early stage surgical trial to resect these regions.
